
How do you open a stuck drawer (translatory motion joint)?

You have to tilt / lift / wiggle the drawer, but the main action is by gliding it back and forth.
How about a stuck hinged door (rotary motion joint)?

Do you use the same method of opening the drawer (gliding the joint) to open the door? I don’t think so. You have to push/pull the stuck door itself (angular motion) while moving (displacing/shifting) the door hinge to open the door.

How about in a human body joint?
Most of the human joints are angular motion(rotary motion) joints since almost all joint have axis.
Have you ever questioned why we glide linearly on our peripheral joint?
Current Joint Mobilization Controversy
Current joint mobilization is translatoric (linear) gliding technique performed on a rotary motion joint(movement around an axis), and there is much debate in the literature about determining the direction of joint mobilization. The joint axis direction of movement in osteokinematics is different from Kaltenborn’s Convex-Concave rule of determining gliding direction in arthrokinematics.
Osteokinematic view
The translatoric (linear) gliding technique is applied on limited rotary motion joint. We know without a doubt that rotary motion is limited, but we don’t know whether the joint axis shift (movement) is limited or not. Why do we mobilize the joint axis only and do not mobilize the limited rotation? Isn’t the rotary motion joint restriction due to limited rotation?
Arthrokinematic view
The translatoric (linear) gliding technique is applied on limited roll and curved glide motion which is rotation. Why do we only linearly glide on rotation motion?
When the translatoric gliding technique is applied on a convex surface or a concave surface, a single point on the convex surface contacts multiple points on the concave surface. This is far different than the normal arthrokinematic rotation on convex and concave surfaces. Rotary motion occurs when a single point on concave surface contact multiple points on convex surfaces regardless of joint congruency (arthrokinematic rotation).
Joint motion
(Arthrokinematics)


A single point on concave surface contact multiple points on convex surfaces
Translatoric glide
(Arthrokinematics)


A single point on convex surface contacts multiple points on concave virtual surface.
Is roll-gliding really rotation (rotatory movement of the joint)?

There are two ways of going down hill. One is going down the slope, the other is going down vertically then going horizontally on the bottom of the slope.
Can you say "I'm skiing down the slope" if you are going down vertically and walking on the bottom of the slope?
Most of our human body joints are rotary motion joint and rotation occurs in rotary motion joint. However as you know rotation is divided into roll-glide in arthrokinematics, and we glide the joint based on Mr. Freddy Kaltenborn's joint restriction theory(glide impairment). Is rotation really as same as roll-glide?
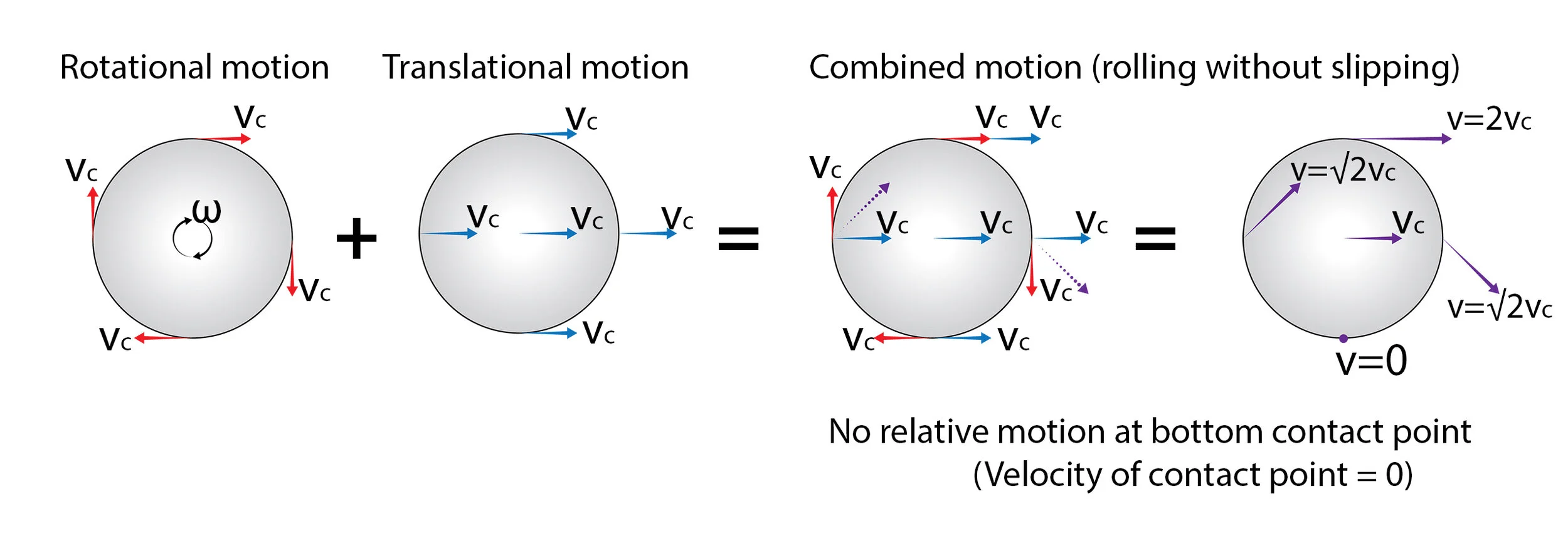
Rolling without slipping in Rigid body kinematics is a roll in arthrokinematics. This rolling without slipping motion is the combined motion of rotation and translation(glide), it is completely different then the convex-concave rule (roll and slide movement concept). Why is the same rolling motion explained differently between rigid body kinematics and arthrokinematics?
Dr. Kim's Joint Restriction Theory and Mobilization Concept
Dr. Kim's theory of joint restriction is due to rotation impairment with possible impaired joint shift and applying the technique has to be rotation based and not translatoric gliding based technique.
Conventional joint mobilization is a translatoric gliding technique based on Kaltenborn's theory that the joint restriction is from impaired gliding.
What is Angular Joint Mobilization® (AJM)?
Angular Joint Mobilization® is a rotary joint mobilization technique with joint shift that follows joint biomechanics, not like traditional translatoric joint mobilization technique.
Dr. Kim’s concept of joint mobilization is a rotary technique that has to be applied to restricted rotary motion joint instead of translatoric gliding technique. During joint mobilization, angular movement (rotary motion or curved glide motion in the joint) should be considered the major joint mobilization and joint shift on the axis or on the articular joint surface should be considered the assistive joint mobilization. This insures that the joint structure will be mobilized along the joint surface, stretching other structures effectively and will allow the joint to regain full range of motion more easily since this Angular Joint Mobilization® matches the osteokinematics and arthrokinematics.
Applying the Angular Joint Mobilization® Technique:
Step 1. Primary Joint Mobilization - arc of movement utilizing a long lever arm as much as possible to the end range with overpressure to tolerance. This is passive most of the time.
Step 2. Joint Shift (Assistive joint mobilization) - sustained pressure, or over pressure (anterior shift / posterior shift / superior shift / inferior shift / medial shift / lateral shift / rotational shift)
Step 3. Combined movement (Advanced) – Physiological movement to move all direction w/o limitations.

Knee flexion Angular Joint Mobilization - Anterior and inferior shift
Angular Joint Mobilization® Direction (Primary joint mobilization)
It follows the direction of limited lever arm motion (e.g. if knee flexion is limited, then the direction of primary joint mobilization is flexion.).
Angular Assistive joint Mobilization Direction
The direction of Angular Assistive joint mobilization can be affected by the joint space, joint surface, capsule, ligaments, muscle (tendon), loss of or defect in the stabilizing mechanism in the joint, pain, muscle spasm, loss of proprioception associated with dysfunction, imbalance/incoordination of the musculature, etc.
The joint shift (angular assistive joint mobilization) direction doesn't follow Kaltenborn’s convex concave rule at all.
Helpful tips for determining the angular assistive joint mobilization direction:
Always apply Primary Joint Mobilization (arc of movement with over pressure) before apply shift and see whether ROM increase or not.
Apply shift (sustained glide most of the time or rotation from mid range (slack) to pathological end range while arc of movement on the lever arm is applied
Identify the angular assistive joint mobilization direction that provides the most increased ROM
Identify the most restricted angular assistive joint mobilization(shift) direction and provides the most joint structure stretching and increased ROM. (If it is hard to identify this direction, and then simply ask the patient which one produces the most stretching and lesser pain.)
The joint structure has to be freely moving in all accessory movement directions at every angle of the lever arm.
Shift in the opposite direction after mobilizing in one direction. (For ex: Glenohumeral joint abduction joint mobilization with posterior shift then abduction mob with anterior shift.)
Avoid impingement, anatomical limit, or severe pain
The Angular Joint Mobilization® Treatment Plane is not parallel to the concave joint surface because concave joint surface is not flat surface(curved surface) and convex-concave joint is a rotary motion joint not a translatoric motion joint.
Primary Joint Mobilization is applied at the pathological limit, but stops before the anatomical limit of the range of motion. This therapeutic technique should not produce sharp pain, even with over pressure
Grade 0 - Rotary oscillations are applied before the start of pathological limit.
Grade I (In a painful joint) - Rotary oscillations are applied with slight overpressure at the beginning of pathological limit. Like a swinging pendulum, the joint tissues are on slack at the beginning to mid part of the arc of movement. and joint stretching occurs towards the end.
Grade II - Rotary oscillations are applied with overpressure, stop before the end of pathological limit. Joint tissues are slack at the beginning of the arc of movement and joint stretching occurs from mid to end of the arc of movement.
Grade III (In a non-painful joint) - Rotary oscillations are needed with more over pressure to the end of pathological limit.
Assistive joint mobilization(Shift)- Sustained pressure / Overpressure:
(Glide /rotation / spin / compression / distraction)
Sustained pressure (Shift) – Apply pressure at the end of pathological accessory range to tighten the tissues and sustain
Overpressure: Apply overpressure at the end of pathological accessory range to stretch while Primary Joint Mobilization are applied and then come back to the slack position
Differences between Angular Joint Mobilization® and MWM (by Brian Mulligan)
Angular Joint Mobilization®
Can be painful within patient tolerance
Accessory joint mobilization is not parallel to the concave joint surface
Can apply any accessory movement (glide/rotation/spin/compression/distraction) – Multidirectional movement
Usually passive but can be active, active with end range overpressure, combined with muscle energy techniques
Mobilizations with movement
Pain free
Accessory joint mobilization is parallel to the concave joint surface
Only one direction of accessory joint glide.
Active or resisted with end range overpressure
Angular Joint Mobilization® indications: All joints with restricted range of motion regardless if capsular or non capsular patterns exist, prosthetic joints (e.g. Total knee arthroplasty, etc.).
Angular Joint Mobilization® contraindications are consistent with the general contraindications for conventional joint mobilizations. These are well described by other authors in various manual therapy books and from the internet.
Inferior Tibiofibular joint ankle dorsiflexion AJM Distraction/Splaying
Talocrural Joint Dorsiflexion Angular Joint Mobilization®(AJM) Anterior Shift